Icd 10 Hernia Nukleus Pulposus
 Retrolisthesis Wikipedia
Retrolisthesis Wikipedia
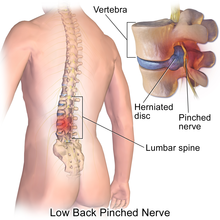
herniation of nucleus pulposus
A history is obtained of any unilateral low back pain that radiates to the buttocks, legs, and feet. Almost all herniations occur in the lumbar and lumbosacral region; 8% in the cervical region and only 1% to 2% in the thoracic region. When herniation follows trauma, the patient may report sudden pain, subsiding in a few days, then a dull, aching sciatic pain in the buttocks that increases with Valsalva's maneuver, coughing, sneezing, or bending. The patient may also complain of muscle spasms accompanied by pain that subsides with rest. The health care professional inspects for a limited ability to bend forward, a posture favoring the affected side, and decreased deep tendon reflexes in the lower extremity. In some patients, muscle weakness and atrophy may be observed. Palpation may disclose tenderness over the affected region. Tissue tension assessment may reveal radicular pain from straight leg raising (with lumbar herniation) and increased pain from neck movement (with cervical herniation). Thorough assessment of the patient's peripheral vascular status, including posterior tibial and dorsalis pedis pulses and skin temperature of the arms and legs, may help to rule out ischemic disease as the cause of leg numbness or pain.
The patient is prepared for diagnostic testing by explaining all procedures and expected sensations. Tests may include radiographic studies of the spine (to show degenerative changes and rule out other abnormalities), myelography (to pinpoint the level of herniation), computed tomography scanning (to detect bone and soft tissue abnormalities and possibly show spinal compression resulting from the herniation), magnetic resonance imaging (to define tissues in areas otherwise obscured by bone), electromyography (to confirm nerve involvement by measuring the electrical activity of muscles innervated by the affected nerves), and neuromuscular testing (to detect sensory and motor loss as well as leg muscle weakness).
Pain and its management are often crucial elements of care; levels of pain are monitored, prescribed analgesics are administered, the patient is taught about noninvasive pain relief measures (such as relaxation, transcutaneous nerve stimulation, distraction, heat or ice application, traction, bracing, or positioning), and the patient's response to the treatment regimen is evaluated. During conservative treatment, neurological status is monitored (esp. in the first 2 to 3 weeks after beginning treatment) for signs of deterioration, which may indicate a need for surgery. Neurovascular assessments of the patient's affected and unaffected extremities (both legs or both arms) are performed to check color, motion, temperature, sensation, and pulses. Vital signs are monitored, bowel sounds are auscultated, and the abdomen is inspected for distention. The disorder and the various treatment options are explained to the patient, including bedrest and pelvic (or cervical) traction, local heat application, a physical therapy designed exercise program, muscle-relaxing and anti-inflammatory drug therapy, injection of local anesthetic and steroid drugs, acupuncture, and surgery.
Both the patient and family are encouraged to express their concerns about the disorder; questions are answered honestly, and support and encouragement are offered to assist the patient and family to cope with the frustration of impaired mobility and the discomfort of chronic back pain. The patient is encouraged to perform self-care to the extent that immobility and pain allow, to take analgesics before activities, and to allow adequate time to perform activities at a comfortable pace.
Walking and gentle stretching are encouraged as part of daily exercise during conservative therapy. If the patient is restricted to bedrest (or in traction), the patient should increase fluid intake and use incentive spirometry to avoid pulmonary complications. Skin care and a fracture bedpan are provided if the patient is not permitted bathroom or commode privileges.
For patients who require surgery, the patient is prepared physically and psychologically for the specific procedure (laminectomy, spinal fusion, microdiskectomy) and postoperative care regimen, and informed consent is obtained. The patient may donate blood prior to surgery for later autotransfusion as needed.
Postoperative Care: Bedrest is enforced for the prescribed period, the blood drainage system in use is managed, and the amount and color of drainage are documented. Any colorless moisture or excessive drainage should be reported; the former may indicate cerebrospinal fluid leakage. A log-rolling technique is used to turn the patient from side to side, and the patient is taught how to turn in this manner when moving about or getting up from bed at home. Analgesics are administered as prescribed, esp. 30 min before early attempts at mobilization. The health care professional assists the patient with prescribed mobilization. Depending on the surgery required, the patient may require a back brace (individually fitted) for a period of time after surgery, and this is carefully fitted and the patient taught about its use.
Before discharge, proper body mechanics are reviewed with the patient: bending at the knees and hips (never the waist), standing straight, and carrying objects close to the body. The patient is advised to lie down when tired and to sleep on the side or back (never on the abdomen) on an extra-firm mattress or a bed board. All prescribed medications are reviewed, including dosage schedules, desired actions, and adverse reactions to be reported. Referral for home health care or physical/occupational therapy may be necessary to help the patient manage activities of daily living.
Gallery Icd 10 Hernia Nukleus Pulposus
 Spinal Disc Herniation
Spinal Disc Herniation
 Spinal Disc Herniation Wikipedia
Spinal Disc Herniation Wikipedia
 Icd Hnp Lumbar Docx Vertebral Column International
Icd Hnp Lumbar Docx Vertebral Column International
 The New Rating System For Back And Neck Spinal Disability
The New Rating System For Back And Neck Spinal Disability
 Low Back Pain Wikipedia
Low Back Pain Wikipedia
 Cox Technic A Discussion Place For Spinal Pain Management
Cox Technic A Discussion Place For Spinal Pain Management
Nomenclature And Classification Of Lumbar Disc Pathology
Link International Statistical Classification Of Diseases
 Glen Ellyn Disc Pain Disc Herniation Disc Buldge
Glen Ellyn Disc Pain Disc Herniation Disc Buldge
 Back Pain Treatment Video Download Back Pain Icd 10
Back Pain Treatment Video Download Back Pain Icd 10
 Kode Diagnosa Bpjs
Kode Diagnosa Bpjs
2017 Icd 10 Common Add Codes List Updated 1 09 17 Human
 Kode Diagnosa Bpjs
Kode Diagnosa Bpjs
 Sciatica
Sciatica
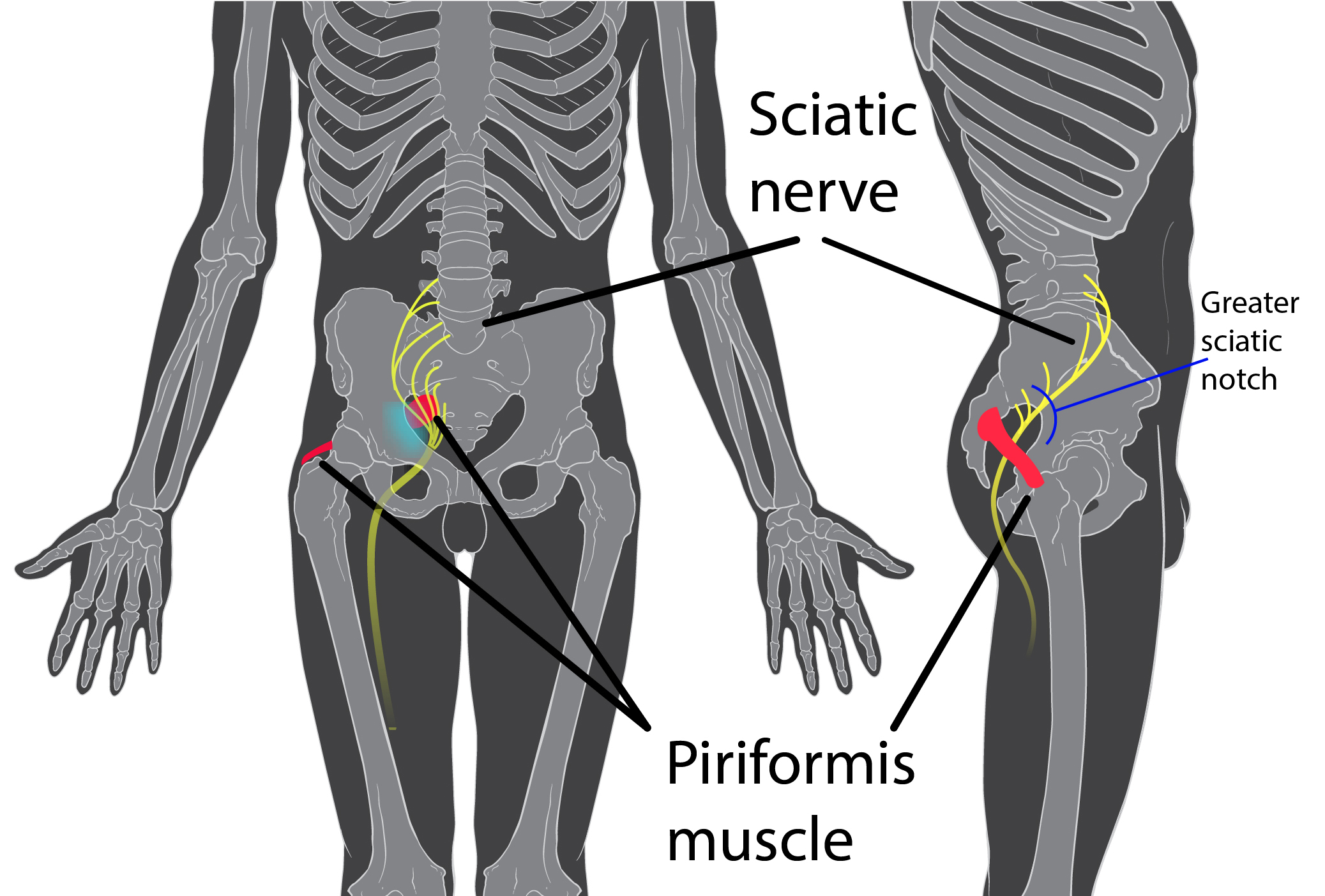 Piriformis Syndrome Wikipedia
Piriformis Syndrome Wikipedia
 Homepage The Pain Source Makes Learning About Pain Painless
Homepage The Pain Source Makes Learning About Pain Painless
 Icd 10 Cm Pcs Part 65 Question Answer Codebusters
Icd 10 Cm Pcs Part 65 Question Answer Codebusters
 Getting To The Backbone Of Spinal Coding In Icd 10 Pcs Pdf
Getting To The Backbone Of Spinal Coding In Icd 10 Pcs Pdf
 Stay Current With Spine Procedural Coding Aapc Knowledge
Stay Current With Spine Procedural Coding Aapc Knowledge
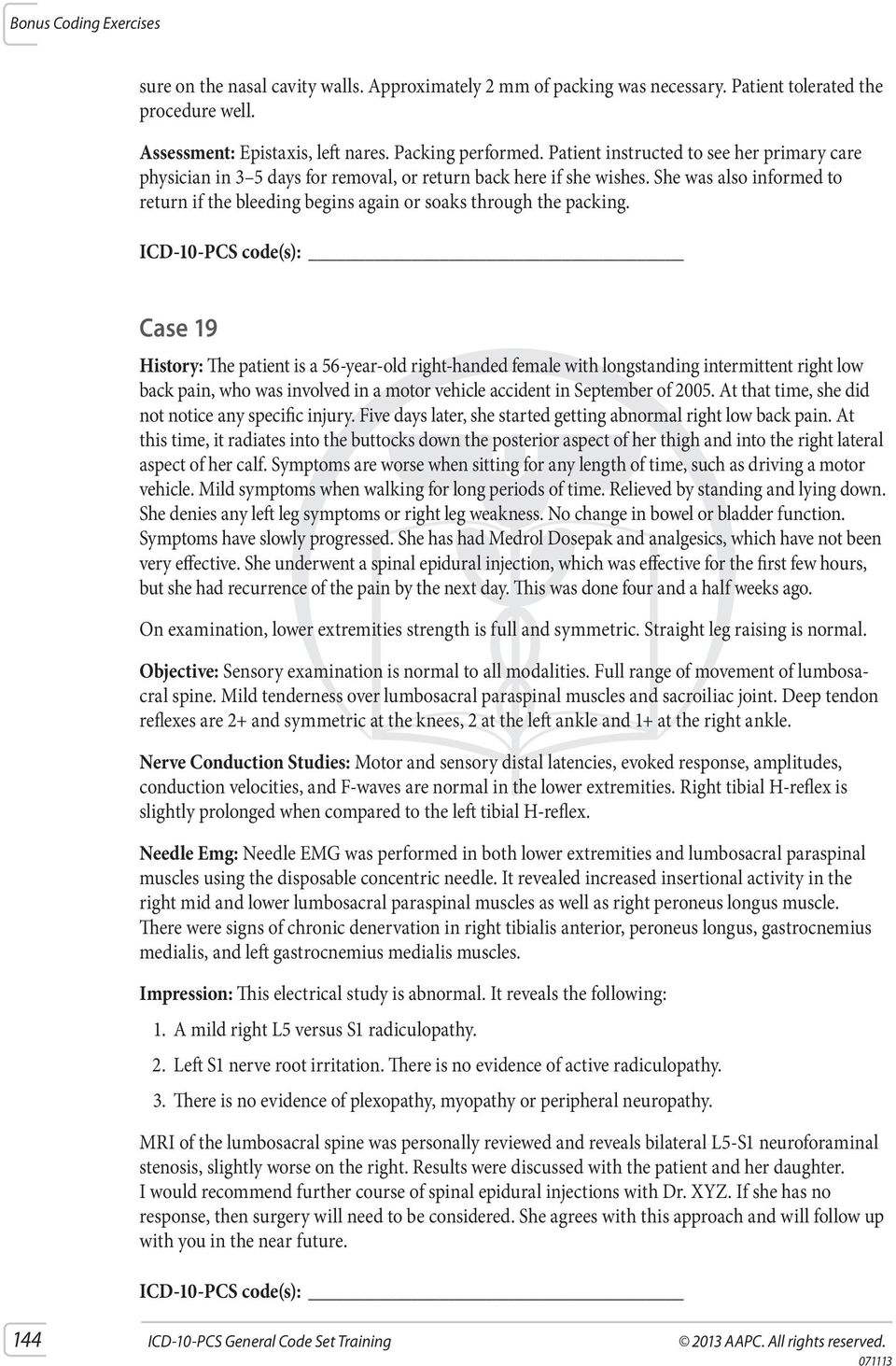 Icd 10 Pcs Code Set Training General Part 6 Pdf Free
Icd 10 Pcs Code Set Training General Part 6 Pdf Free
Nomenclature And Classification Of Lumbar Disc Pathology
Cervical Disc Herniation Icd 10
 Icd 10 International Statistical Classification Of Diseases
Icd 10 International Statistical Classification Of Diseases
Genome Wide Meta Analysis Of 158 000 Individuals Of European
 Study Flowchart Ldh Lumbar Disc Herniation Lss Lumbar
Study Flowchart Ldh Lumbar Disc Herniation Lss Lumbar
Nomenclature And Classification Of Lumbar Disc Pathology
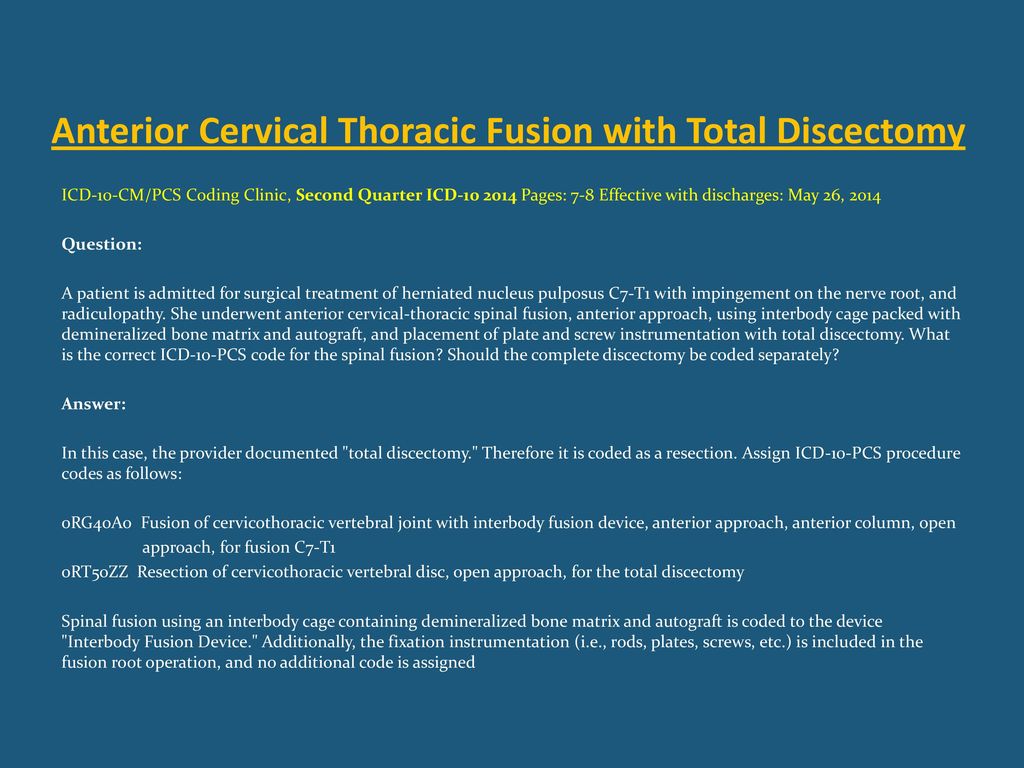 Spinal Procedure Coding In Icd Ppt Download
Spinal Procedure Coding In Icd Ppt Download







0 Response to "Icd 10 Hernia Nukleus Pulposus"
Post a Comment