Kode Icd 10 Stroke
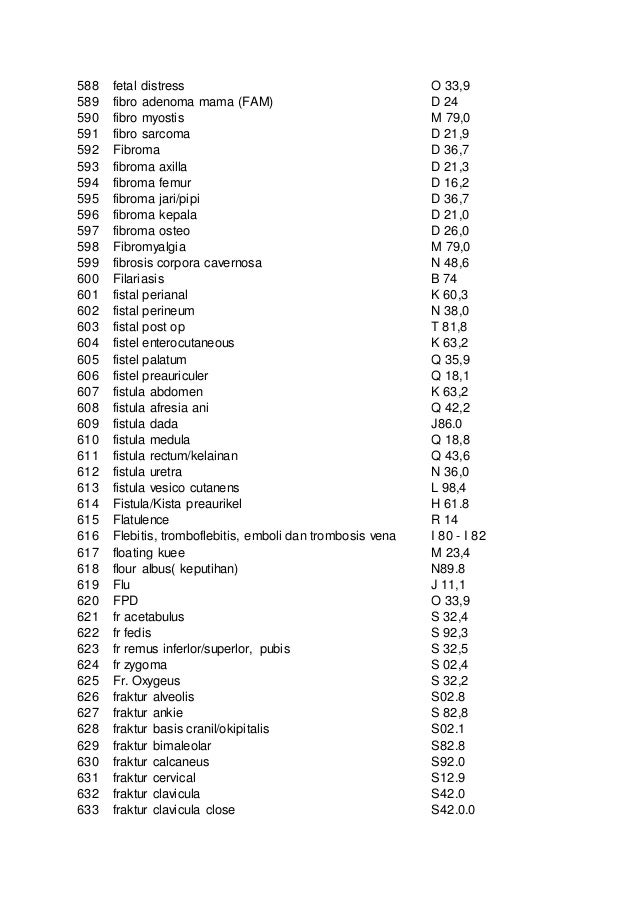 Kode Pintar Icd 10
Kode Pintar Icd 10
ICD-10-CM coma, stroke codes require more specific documentation
Want to receive articles like this one in your inbox? Subscribe to JustCoding News: Inpatient!
A quick glance at ICD-9-CM and ICD-10-CM stroke and coma codes reveals many similarities and some important differences.
How ICD-10 stroke codes are organized The 2013 ICD-10-CM Table of Diseases organizes cerebrovascular disease codes as follows:
- I60-I62: Non-traumatic intracranial hemorrhage (i.e., spontaneous subarachnoid, intracerebral, or subdural hemorrhages)
- I63: Cerebral infarctions (i.e., due to a vessel thrombosis or embolus)
- I65-I66: Occlusion and stenosis of cerebral or precerebral vessels without infarction
- I67-I68: Other cerebrovascular diseases
- I69: Sequelae of cerebrovascular disease (late effect)
Note that some neurologic manifestations of cerebrovascular disease, such as transient cerebral ischemic attacks and related syndromes (G45), are classified elsewhere.
Greater specificity for strokes ICD-10-CM stroke codes are more specific than their ICD-9-CM counterparts. First, codes I60-I62 specify the location or source of a hemorrhage as well as its laterality. For example, ICD-10-CM code I60.11 denotes nontraumatic subarachnoid hemorrhage from right middle cerebral artery.
A CT scan usually indicates the specific location of a hemorrhage, says Alice Zentner, RHIA, director of auditing and education at TrustHCS in Springfield, Mo. "Hopefully, the physician will bring this information forward into his or her progress notes," she says.
Second, code category I63 specifies the following:
- Cause of the ischemic stroke (e.g., thrombosis, ¬embolus, or unspecified)
- Specific location and laterality of the occlusion (i.e., specific artery)
For example, ICD-10-CM code I63.331 denotes cerebral infarction due to thrombosis of right posterior cerebral artery.
Zentner says that coders must be able to differentiate the following terms when reporting a code from category I63-I65:
- Stenosis-narrowing of the artery
- Occlusion-Complete or partial obstruction
- Thrombus-Solid mass of platelets or fibrin that forms and remains in a blood vessel (stationary blood clot)
- Embolism-Blood clot that travels from the site where it formed to another location in the body
Coders should also be able to distinguish cerebral and precerebral arteries because ICD-10-CM codes make this distinction, says James S. Kennedy, MD, CCS, CDIP, managing director at FTI Consulting in Atlanta. Precerebral arteries include the vertebral, basilar, and carotid arteries and their branches. The cerebral arteries include the anterior, middle, and posterior cerebral arteries and their branches. Third, code category I69 specifies the type of stroke that caused the sequelae as well as the residual condition itself. For example, code I69.01 denotes cognitive deficits after nontraumatic subarachnoid hemorrhage. In ICD-9-CM, code 438.xx simply denotes the residual condition-not the type of stroke that caused the condition. Coders can report a code from category I69 in conjunction with a condition classifiable to code category I60-I67 if the patient has a current cerebrovascular disease and deficits from an old cerebrovascular disease. Coding guidelines also state that the neurological deficits caused by a stroke may be present from the onset of a stroke or arise at any time after the onset of the stroke. Note that codes in category I69 are exempt from POA reporting. When a patient has a history of cerebrovascular disease without any neurologic deficits, coders should report code Z86.73 (personal history of transient ischemic attack, and cerebral infarction without residual deficits) and a code for the cerebral infarction without residual deficits (not code I69), according to 2012 ICD-10-CM guidelines.
Reporting bilateral hemorrhages If a patient suffered bilateral nontraumatic intracerebral hemorrhages, coders should report code I61.6 (nontraumatic intracerebral hemorrhage, multiple localized).
Conversely, if a physician documents bilateral nontraumatic subarachnoid hemorrhage sites, coders must report an ICD-10-CM code for each side. ICD-10-CM guidelines state that if the patient has a bilateral condition-and no bilateral ICD-10-CM code exists-coders should assign separate codes for the left and right sides.For example, in the rare event that a patient suffers a nontraumatic subarachnoid hemorrhage of both anterior communicating arteries, assign both:
- I60.21, nontraumatic subarachnoid hemorrhage from right anterior communicating artery
- I60.22, nontraumatic subarachnoid hemorrhage from left anterior communicating artery
However, coders should note that code categories I65-I66 include bilateral codes. Therefore, if a patient has bilateral stenosis of the vertebral arteries, coders should assign I65.03-not I65.01 and I65.02 to denote the right and left vertebral arteries, respectively.
Reporting intraoperative and postprocedural strokes Unlike ICD-9-CM, ICD-10-CM distinguishes the following:
- Intraoperative stroke during cardiac surgery (I97.810) or during other surgery (I97.811)
- Postprocedural stroke during cardiac surgery (I97.820) or during other surgery (I97.821)
"If a stroke occurs in the setting of an operation, a query is needed to determine if the stroke occurred during or after surgery," says Kennedy.
Coma codes The most noticeable difference between ICD-9-CM code 780.01 (coma) and its ICD-10-CM counterpart (code category R40.2) is that the latter incorporates the Glasgow Coma Scale (GCS), a neurological scale that captures a patient's conscious state for initial and subsequent assessment.
"It really shows the condition of the patient and the severity of the event," says Zentner. "If reported at different intervals, it shows the patient's progress and response to treatment." Coders may report the GCS with any appropriate illness. The coma scale codes should be sequenced after the diagnosis code(s). The GCS may be coded based on an aggregate score (code R40.24, GCS total score), or based on its individual components. Code R40.24 is appropriate when only the total score-and not the individual components-are documented. When the individual components are documented, coders may report theGCS based on the components. However, they must report a code from each of the following subcategories:
- R40.21: Eye response (eyes never open or eyes open to pain, sound, or spontaneously)
- R40.22: Best verbal response (clarity of words ¬incomprehensible, inappropriate, confused, oriented)
- R40.23: Best motor response (voluntary and ¬involuntary responses [extension, flexion, abnormal, obeys commands])
If a physician doesn't document the GCS-or documents only a portion of it-coders must report R40.244 (other coma, without documented Glasgow coma scale score, or with partial score reported). Codes R40.21-R40.23 require a seventh character to denote when the scale was recorded (i.e., unspecified time, in the field [EMT or ambulance], upon arrival at the ED, at hospital admission, or 24 hours or more after admission). Coders must report codes for all three components, and they must ensure that the seventh character matches for all three, says Kennedy. Coders also should note that hospitals may report the GCS at multiple intervals and that physician and EMT documentation must support code assignment, he says. "Facilities that have a trauma registry will certainly want to report these codes," says Zentner. "If the center wants to follow the patient and see how he or she is progressing, they may want to report several codes." Educating ED physicians about documentation of coma scale scores and the new codes is important. Hospitals should consider revising templates so they incorporate this information, she says. Separate symptoms and combination codes Coders should search the ICD-10-CM Alphabetic Index for codes that automatically incorporate coma in their descriptions. For example, code E11.641 denotes Type 2 diabetes mellitus with hypoglycemia with coma. Assigning ICD-10-CM code R40.20 (coma, unspecified) as an additional code would be appropriate because combination code E11.641 includes the coma (symptom) as an integral component.
Editor's note: Access the most recent version ofICD-10-CM and the 2012 ICD-10-CM guidelines, online. This article was originally published in the September issue of Briefings on Coding Compliance Strategies. Email your questions to Senior Managing Editor Michelle A. Leppert, CPC, at mleppert@hcpro.com.
Want to receive articles like this one in your inbox? Subscribe to JustCoding News: Inpatient!
Gallery Kode Icd 10 Stroke
 Acute Blood Loss Anemia Icd 10
Acute Blood Loss Anemia Icd 10
 How To Code Sequela Of Cva In Icd 10 Home Health Coding Tip By Pps Plus September 2017
How To Code Sequela Of Cva In Icd 10 Home Health Coding Tip By Pps Plus September 2017
![]() Common Icd 10 Codes For Otolaryngology Icd 10 Code Lookup
Common Icd 10 Codes For Otolaryngology Icd 10 Code Lookup
 Pdf Coding Geriatric Syndromes How Good Are We
Pdf Coding Geriatric Syndromes How Good Are We
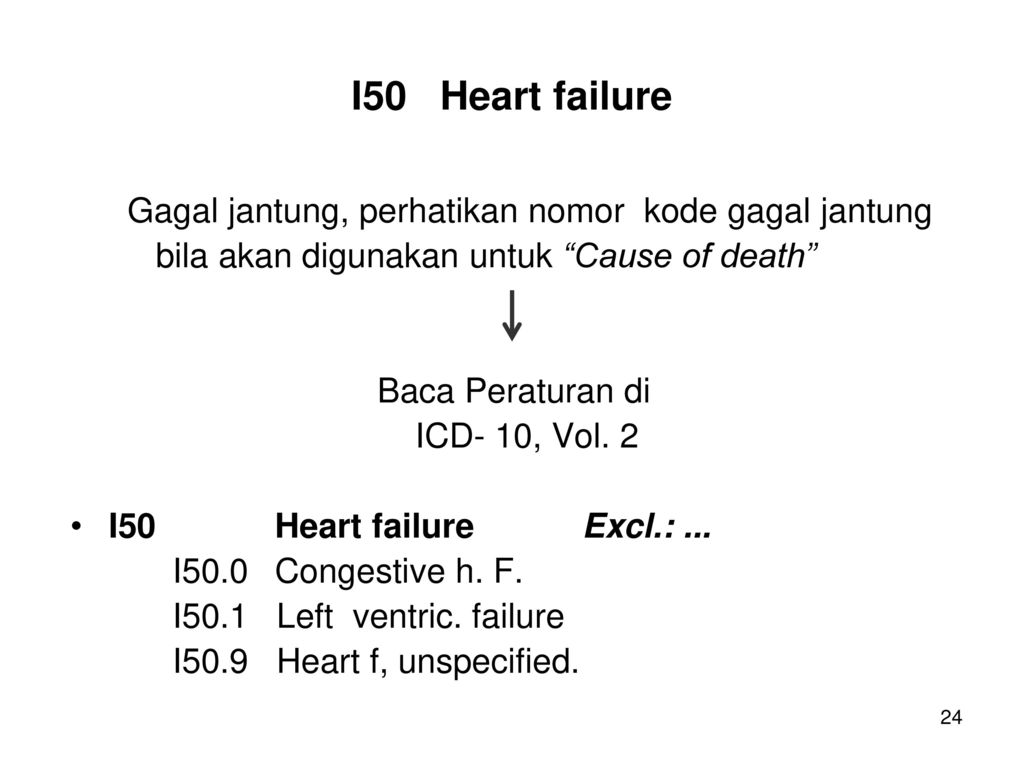 Kkpmt I 10 Icd 10 Chapter Ix Diseases Of The Circulatory
Kkpmt I 10 Icd 10 Chapter Ix Diseases Of The Circulatory
 Icd 10 Residuals Of Cva And Traumatic Brain Bleeds
Icd 10 Residuals Of Cva And Traumatic Brain Bleeds
 Icd Coding For Epilepsy Past Present And Future A Report
Icd Coding For Epilepsy Past Present And Future A Report
 Icd 10 Codes Have You Made These Diagnoses Medical Bag
Icd 10 Codes Have You Made These Diagnoses Medical Bag
 Guide For Icd 10 S And Ambulance Services
Guide For Icd 10 S And Ambulance Services
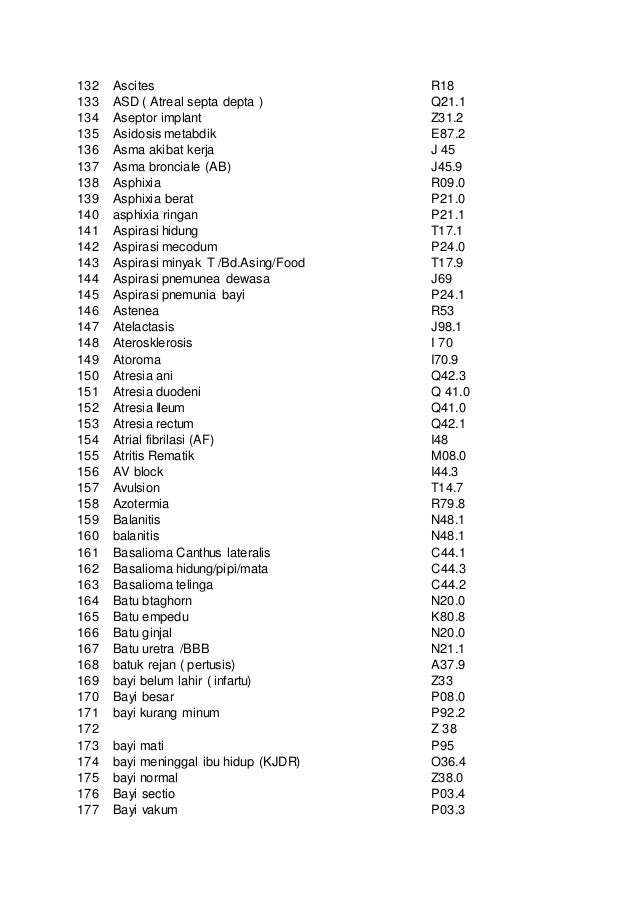 Kode Pintar Icd 10
Kode Pintar Icd 10
 Kode Icd 10 Diabetes Melitus E11 6 Icd 2019 09 28
Kode Icd 10 Diabetes Melitus E11 6 Icd 2019 09 28
 Kode Icd 10 Hypertension
Kode Icd 10 Hypertension
 Icd 10 Physical Therapy Guide To Icd 10 Codes Webpt
Icd 10 Physical Therapy Guide To Icd 10 Codes Webpt
2020 Icd 10 Cm Diagnosis Codes Related To Hearing And
Untitled
 Vulnus Icd 10 Provy
Vulnus Icd 10 Provy
 Cbd Tumor Icd 10 2020
Cbd Tumor Icd 10 2020
Icd 10 International Statistical Classification Of Diseases
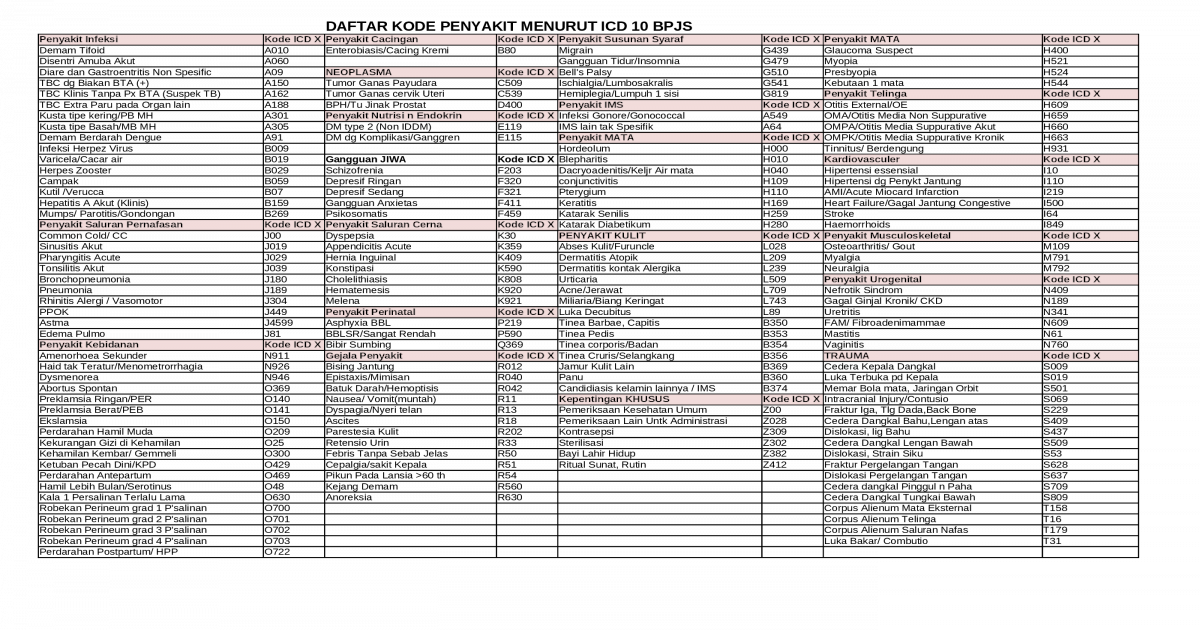
 Doc Kode Icd X Stefan Azzwa Academia Edu
Doc Kode Icd X Stefan Azzwa Academia Edu
 Icd 10 Archives Hiacode
Icd 10 Archives Hiacode
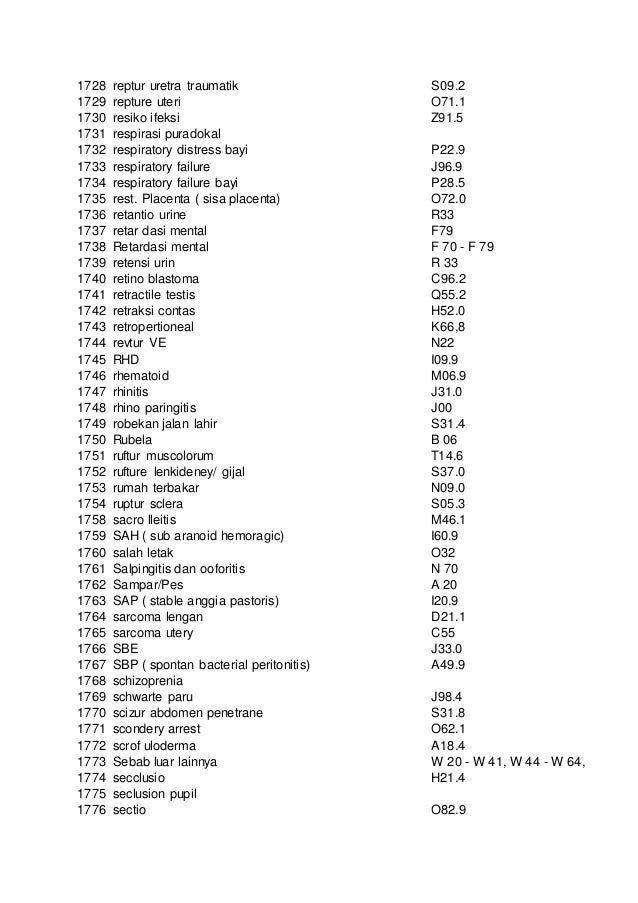 Kode Pintar Icd 10
Kode Pintar Icd 10
 Draft Icd 10 Clinical Modification Code Sets Pdf Free
Draft Icd 10 Clinical Modification Code Sets Pdf Free
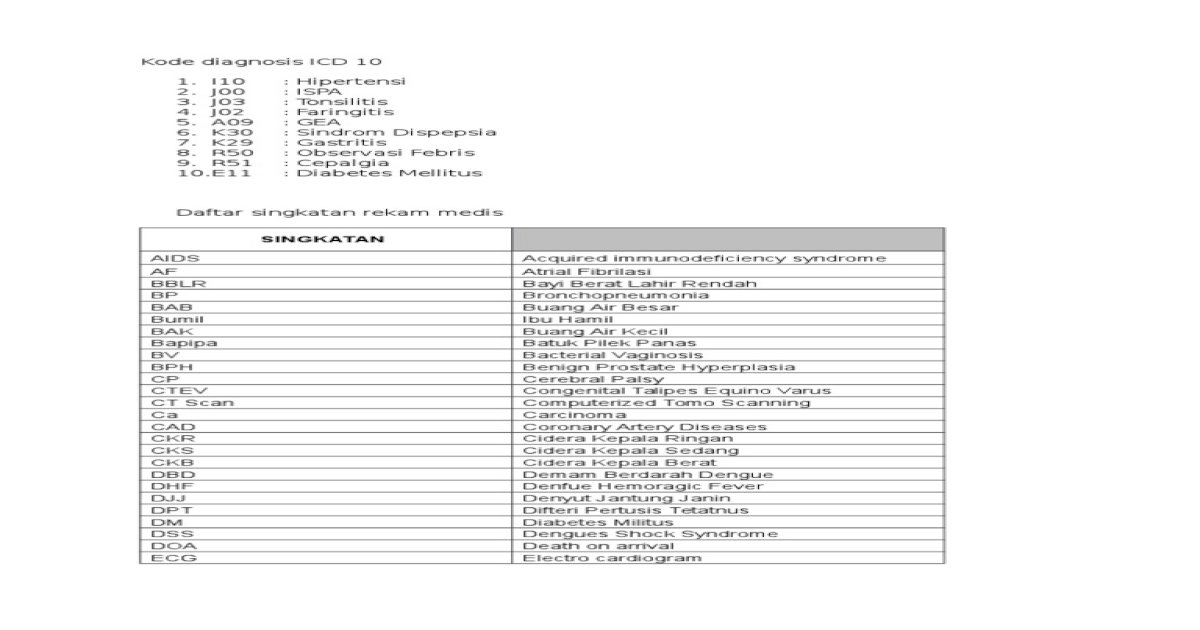 Diagnosis Icd 10 Dan Daftar Singkatan
Diagnosis Icd 10 Dan Daftar Singkatan
 Icd 10 Print Ok
Icd 10 Print Ok
 Kode Icd 10 Jlk9v6m6z545
Kode Icd 10 Jlk9v6m6z545
 Icd 10 Coding For Hypertension And Heart Disease
Icd 10 Coding For Hypertension And Heart Disease








0 Response to "Kode Icd 10 Stroke"
Post a Comment