Theory Of Reasoned Action
 Theory Of Reasoned Action And Theory Of Planned
Theory Of Reasoned Action And Theory Of Planned
A Reasoned Action Approach to Health Promotion
Martin Fishbein, PhD
This article describes the integrative model of behavioral prediction (IM), the latest formulation of a reasoned action approach. The IM attempts to identify a limited set of variables that can account for a considerable proportion of the variance in any given behavior. More specifically, consistent with the original theory of reasoned action, the IM assumes that intentions are the immediate antecedents of behavior, but in addition, the IM recognizes that environmental factors and skills and abilities can moderate the intention-behavior relationship. Similar to the theory of planned behavior, the IM also assumes that intentions are a function of attitudes, perceived normative pressure and self-efficacy, but it views perceived normative pressure as a function of descriptive as well as of injunctive (i.e., subjective) norms. After describing the theory and addressing some of the criticisms directed at a reasoned action approach, the paper illustrates how the theory can be applied to understanding and changing health related behaviors.
I think that it is safe to say that almost everyone reading this article would like to develop interventions to improve medical decision making and the public's health. However, as we all know, not all interventions are effective; and even worse, some may actually be counterproductive.1,2 What behavioral science theory and research can do is provide guidelines for developing effective behavior change programs. Clearly, the more one knows about the factors that underlie the performance (or nonperformance) of any given behavior, the more likely it is that one can design a successful intervention to change or reinforce that behavior. In this article, I describe a theoretical approach to the prediction and understanding of human behavior with a view to its application in medical and health contexts. More specifically, I describe an integrative model (IM) for behavioral prediction.3 This model represents the latest formulation of the reasoned action approach, which includes the theory of reasoned action4,5 and the theory of planned behavior.6 Both theories have been supported by extensive empirical evidence.7-10 What the reasoned action approach attempts to do is to identify a relatively small set of variables that can account for a substantial proportion of the variance in any given behavior.
This set of variables can be applied to actions by health care providers, whose behaviors should change over time as new evidence to alter recommended practice becomes available, as well as to actions by patients and members of the public who are increasingly asked to participate in shared decision making and in preventive health actions, such as engaging in exercise or quitting smoking. Although there are certainly differences between providers and patients in decision making, there are also fundamental similarities,11 which are focused on here. Thus, the purview of a reasoned action approach extends from the physician deciding whether medical or surgical intervention is best for a patient with stable angina to the adolescent deciding whether to have unprotected sex or to use condoms (or to avoid health risks altogether by abstaining from sexual intercourse).
In this article, I first address one of the major criticisms of a reasoned action approach, and then I consider some of the issues involved in applying it to any behavior. In particular, I consider the problem of carefully defining one's behavior of interest as well as the question of correspondence between the measure of behavior and the measures of its predictors. I then describe the IM of behavioral prediction and show how it can be applied to understanding and changing health-related behaviors.
At the simplest level, a reasoned action approach to the explanation and prediction of social behavior assumes that people's behavior follows reasonably from their beliefs about performing that behavior. I recognize, however, that at least some investigators have questioned the basic assumption that human behavior can be described as reasoned.12 According to this critique, theories like reasoned action and planned behavior are too rational, failing to take into account emotions, compulsions, and other noncognitive or irrational determinants of human behavior.13-17
What these critics have failed to recognize, however, is that a reasoned action approach says nothing about rationality nor does it deny the role of emotions. Indeed, as discussed below, mood and emotion are viewed as “background” variables that may influence one's beliefs about performing the behavior in question. I use the term “reasoned” because it is assumed that as one learns (e.g., forms beliefs) about one's world, one (often automatically) forms attitudes, perceived social norms, and perceptions of control, that in turn (and again, often automatically) influence one's intentions and behaviors. That is, these “higher-order” constructs (e.g., attitudes, norms, intentions) are assumed to follow reasonably from one's beliefs about the world in which one lives. But the beliefs one holds need not be veridical; they may be inaccurate, biased, or even irrational. In addition, as I show below, because the relative importance of attitudes, norms, and self-efficacy as determinants of intentions and behavior vary from person to person and from behavior to behavior, people may sometimes act in ways that seem “irrational” to an outside observer but follow quite reasonably from the beliefs held by the actor.
What I argue in this article is that although there are almost an infinite number of variables that may directly or indirectly influence the performance (or nonperformance) of any behavior, there is a growing consensus that there are only a limited number of variables that need to be considered in order to predict, understand, change, or reinforce a given behavior.18-20 More specifically, I argue that the major variables that need to be considered are intention, attitude, perceived norms, self-efficacy or perceived behavioral control, behavioral beliefs (which are often referred to as cost-benefits or outcome expectancies), normative beliefs, and control beliefs.
Thus, whether one is interested in predicting or understanding why some people get mammograms or colonoscopies while others do not, or why some people eat fruits and vegetables or exercise while others do not, or why some physicians recommend colonos-copies while others do not, a consideration of these 7 variables should not only account for much of the variance in these behaviors but should also provide insight into how to intervene to increase the likelihood that people will arrive at informed decisions to engage in health-protective behaviors.
The first step in using a reasoned action approach is to clearly define (and describe) the behavior or behaviors in which one is interested. Unfortunately, this is not quite as easy as it may appear. First, it is important to recognize that there is a difference between specific behaviors (e.g., walk for 20 minutes 3 times per week), behavioral categories (e.g., exercise, diet), and goals (e.g., lose weight). As I show below, it is much easier to predict whether one will or will not engage in a particular behavior than whether one will or will not engage in a class of behaviors or attain a given goal.a Second, one must also recognize that the definition of a behavior involves 4 elements. More specifically, a behavior can be viewed as involving an action directed at a target, performed in a given context, at a certain point in time.
The definition of action, target, context, and time is somewhat arbitrary. For example, suppose one was interested in predicting whether a man will always use a condom for vaginal sex with his spouse during the next 2 weeks. More specifically, suppose that 2 weeks from now, we ask a respondent whether he did or did not always use a condom for vaginal sex with his spouse during the past 2 weeks. One way of defining this behavior is as follows:
Action: use
Target: condom
Context: vaginal sex with my spouse
Time: always in the past 2 weeks
Alternatively, the behavior could be defined as the following:
Action: using a condom
Target: with my spouse
Context: for vaginal sex
Time: always in the past 2 weeks
Or as the following:
Action: using a condom
Target: unspecified
Context: for vaginal sex with my spouse
Time: always in the past 2 weeks
Irrespective of how one chooses to define a behavior, once that behavior has been defined, a reasoned action approach suggests that a change in any one of these elements changes the behavior under consideration. Thus, from this perspective, one does not perform the same behavior in different contexts but instead performs different behaviors. For example, using a condom with one's spouse is a very different behavior than using a condom with a new or occasional partner. Similarly, using a condom for anal sex is a very different behavior than using a condom for vaginal sex. Equally important, smoking marijuana in the privacy of one's home is a different behavior than smoking marijuana in public, and getting a mammogram at the women's clinic is a different behavior than getting a mammogram at the university hospital.
It is important to recognize that behaviors can be defined from the very specific (e.g., Did you buy [action] Advil [target] at your local Savon pharmacy [context] between 5 and 7 PM on March 3 [time]?) to the most general (e.g., In the past 6 months [time], did you buy [action] a nonprescription pain reliever [target; context left unspecified]?). From this perspective, the level of generality/specificity of any given behavior should be determined by the nature of the problem one is investigating. Thus, sometimes one might be interested in understanding why women did or did not go to a specific venue for a mammogram during a particular time period, while on other occasions one may simply be trying to understand why some women did, while others did not, get a mammogram in the past year.
Irrespective of how the behavior is defined, a reasoned action approach suggests that the single best predictor of whether one will (or will not) perform the behavior in question is the person's intention to perform that behavior. Empirical research over the past 3 decades has led to the recognition that specific behaviors can be predicted with considerable accuracy by assessing intentions to engage in the behaviors under consideration. Intentions can be conceptualized as a readiness to engage in a particular behavior. This readiness to act can find expression in such statements as the following: I will engage in the behavior, I intend to engage in the behavior, I expect to engage in the behavior, I plan to engage in the behavior, I will try to engage in the behavior, and so forth. In other words, as is true of any hypothetical construct, different indicators can be used to assess intention or readiness to perform a given behavior. The essential underlying dimension characterizing an intention, however, is the person's estimate of the likelihood or perceived probability of performing a given behavior. We expect that the higher this subjective probability, the more likely it is that the behavior will in fact be performed.
Some investigators, however, have proposed that rather than being indicators of a single construct, these various measures are better viewed as indicators of different constructs. Thus, for example, a distinction has been made between behavioral intention and behavioral expectation21; more recently, it has also been suggested that intentions (or behavioral expectations) differ in important ways from willingness to perform the behavior.14
Although it may be of interest to consider differences of this kind, the utility of such distinctions for the prediction of behavior is ultimately an empirical question. Available evidence to date suggests that there is little to be gained by the proposed distinctions. For example, most research on this issue has been devoted to the distinction between behavioral intention and behavioral expectation or behavioral self-prediction. In this research, such items as “I intend to . . . .” “I will try to . . . ,” and “I plan to . . .” have been used to assess intentions, while such items as “I expect to . . .” and “I will . . .” have been used to assess behavioral expectations.21 It was hypothesized that behavioral expectations are better predictors of behavior than are behavioral intentions because the former are more likely to take possible impediments to performance of the behavior into account.21,22
While it is true that there are often mean differences between “intentions” and “behavioral expectations,” these 2 measures are very highly correlated, and recent meta-analyses have failed to provide support for the superiority of behavioral expectation measures over measures of behavioral intention as predictors of behavior. For example, in a meta-analysis of studies concerned with the prediction of condom use,23 Sheeran and Orbell10 found no difference in the mean amount of variance accounted for by behavioral expectation (18%) and by behavioral intention (19%), and a meta-analysis of a much broader set of behaviors24 also found no difference in the predictive validity of expectations and intentions.
In a similar fashion, available data also suggest that behavioral willingness is also best viewed as an indicant of the same underlying disposition. Interestingly, Gibbons, Gerrard, Blanton, and Russell14 proposed that measures of willingness were distinct from measures of intentions (or behavioral expectations) because measures of willingness captured nonintentional, reactive, and irrational influences on behavior. This claim seems somewhat unrealistic given how “willingness” is measured. For example, in one of the first studies of “willingness,” willingness to engage in unprotected sex was assessed by asking participants to “imagine being with their boyfriend or girlfriend who wanted to have sex but with no birth control available” and to indicate how likely it was that they would do each of the following: have sex but use withdrawal, not have sex, and have sex without any birth control. It is not at all clear how an average of these 3 conditional intentions can reflect the influence of nonintentional, nonrational factors. Indeed, it appears that people are perfectly capable of reporting how they are likely to react (i.e., what they intend to do) in different hypothetical situations, and just as there is little empirical support for the distinction between intention and behavioral expectation, there is little empirical evidence for a distinction between willingness and either of these intention measures; all 3 are very highly correlated, and all 3 predict behavior about equally well. It is interesting to note that in some of their later studies, Gibbons, Gerrard, and their associates have relied solely on a measure of “willingness” to assess one's propensity to engage in the behavior of interest (i.e., they have dropped a more traditional measure of intention),25,26 or they have used a derived measure that combines willingness and behavioral expectation into a single measure they call “vulnerability.”27 Thus I use the term “intention” to capture one's readiness to engage in a behavior, irrespective of the particular way in which it is measured.
For a measure of intention to correlate closely with behavior, the intention measure must involve exactly the same elements as the behavior itself. The requirement that measures of intention and behavior involve exactly the same action, target, context, and time elements is known as the principle of correspondence or compatibility.28,29 This does not mean that intentions and behaviors should be defined and measured at very specific levels; the principle simply suggests that the 2 variables, intention and behavior, should be measured at equivalent levels of generality or specificity. There is considerable evidence demonstrating that the greater the correspondence between measures of intention and behavior, the higher the correlation between these 2 measures.
Many studies have substantiated the predictive validity of behavioral intentions. When appropriately measured, behavioral intentions account for an appreciable proportion of variance in actual behavior. Meta-analyses covering diverse behavioral domains have reported mean intention-behavior correlations of .47,24,30 .53,22 .45,31 and .62.32 Studies in specific behavioral domains, such as condom use and exercise, have produced similar results, with intention-behavior correlations ranging from .44 to .56.7-10 In a meta-analysis of these and other meta-analyses, Sheeran23 reported an overall correlation of .53 between intention and behavior. It is interesting to note that most of these meta-analyses have not looked at correspondence as a moderator.
A reasoned action approach can be applied equally well to the prediction and understanding of intentions to perform specific behaviors, to engage in categories of behavior, or to reach specific goals; it is important to recognize that although appropriately measured intentions to perform a behavior are very good predictors of the performance or nonperformance of that behavior, intentions to reach goals (e.g., to lose weight; to get an “A” on an examination) are often only weak predictors of actual goal attainment. This is because goal attainment is an outcome that does not necessarily follow from behavioral performance. In addition, it is worth noting that intentions to engage in a category of behaviors may or may not be good predictors of whether one engages in that behavioral category. The problem here concerns the operational definition of the behavioral category. Clearly, if the behavioral category (e.g., dieting or exercising) means something different for an actor than for an observer, the actor might believe she has acted on her intentions while the observer may not. Based on these considerations, it should be clear that the most effective interventions will be those directed at changing specific behaviors rather than those directed at behavioral categories or goals. Thus, changing intentions to practice “evidence-based medicine” or intentions to reach a goal such as “improving quality of care” are unlikely to influence any specific clinical practice. In contrast, increasing intentions to “recommend 81 mg/day of aspirin for all diabetes patients 40 and older” (Kaiser Permanente Care Management Institute 2005) should increase the frequency with which the Kaiser recommendations are put in practice.
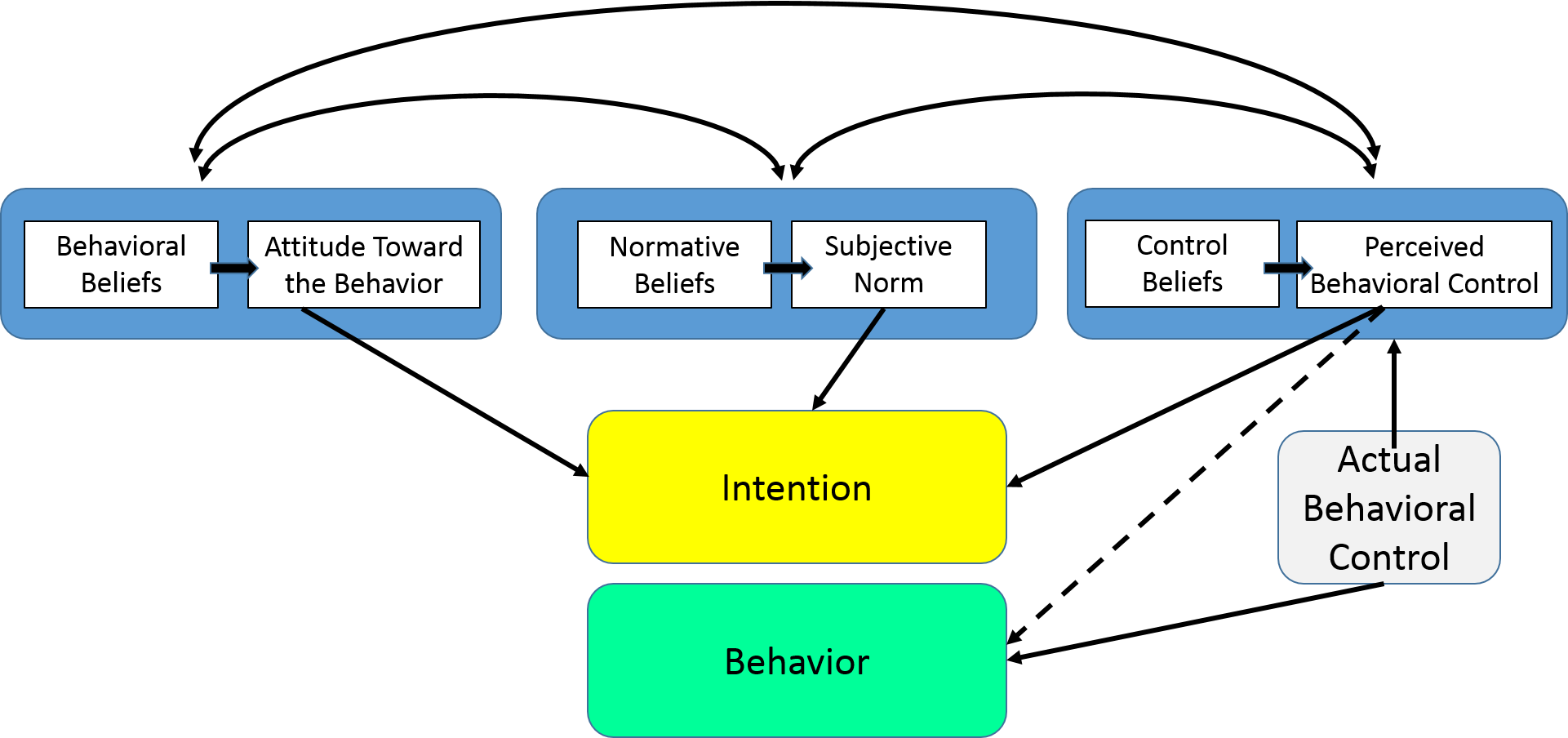
Despite the fact that intentions are probably our best single predictor of whether one will or will not perform a given behavior, intentions do not always predict corresponding behaviors. Even if an individual holds a positive intention, he or she may be unable to act on that intention. Indeed, as can be seen in Figure 1 (which presents the IM of behavioral prediction), several different factors might prevent one from acting upon one's intentions. For example, a person intends to perform a given behavior but when attempting to do so may find that he or she does not have the necessary skills or abilities or may encounter unanticipated barriers or environmental constraints. Clearly, very different interventions are necessary if one has formed an intention but is unable to act on it than if one has little or no intention to perform the behavior.
When people are not performing behaviors we think they should perform, the typical reaction of many health professionals is that people are not performing the “correct” behavior because they do not have all the relevant information or because they have the wrong attitude. Given this explanation, many behavior-change interventions are designed to influence attitudes or to provide appropriate knowledge. More often than not, these interventions do not work because the real problem is that people cannot act on their intentions. If people already intend to perform the behavior in question but are not acting on those intentions, they already have the “right” attitude, and thus it is unlikely that they need more information. The problem is either that they do not have the necessary skills and abilities or that there are internal or external barriers preventing them from acting on their intentions. In these cases, the appropriate intervention is not one designed to impart knowledge or to change attitudes but one directed at skills building or at helping people overcome or avoid barriers.
On the other hand, if people are not performing a behavior because they have little or no intention to do so, the problem is very different. As indicated earlier, according to the IM, there are 3 primary determinants of intention: the attitude toward performing the behavior in question, normative influence or the amount of social pressure one feels vis-à-vis performing the behavior, and one's beliefs that one has the necessary skills and abilities to perform the behavior, even under a number of difficult circumstances—that is, one's feelings of self-efficacy or perceived control over the performance of the behavior. The relative importance of these 3 psychosocial variables as determinants of intention will vary as a function of both the behavior and the population being considered.
That is, there are some behaviors that are almost entirely driven by attitudinal considerations, whereas others may be primarily influenced by normative considerations. And a behavior that is attitudinally driven in one culture or population may be normatively driven in another. In some instances, one or another of the 3 factors (attitude, norm, or perceived behavioral control) may not carry any significant weight in the prediction of intention. When this happens, it merely indicates that for the particular behavior and population under investigation, the factor in question is not an important consideration in the formation of intentions.
Thus, before developing interventions to change intentions, it is important to first determine the degree to which that intention is under attitudinal, normative, or self-efficacy control in the population in question. Once again, it should be clear that very different interventions are needed for attitudinally controlled behaviors than for behaviors that are under normative influence or are strongly related to feelings of self-efficacy or perceived behavioral control. Clearly, one size does not fit all, and interventions that are successful in one culture or population may be a complete failure in another. Thus, for example, following practice guidelines might be most strongly influenced by perceived norms in a nontraditional culture but by attitudes in a traditional one.
But if a behavior is primarily influenced by attitudinal, normative, or control considerations, how does one change these variables? As can be seen in Figure 1, attitudes, perceived norms, and self-efficacy are all, themselves, viewed as functions of underlying beliefs—about the outcomes of performing the behavior in question, about the normative proscriptions and/or behaviors of specific referents, and about specific barriers to behavioral performance. Thus, for example, the more one believes that performing the behavior in question will lead to “good” outcomes and prevent “bad” outcomes, the more favorable one's attitude toward performing the behavior. Algebraically this can be expressed as follows:
where Ab is the attitude toward performing the behavior, bi is the belief that performing the behavior will lead to outcome i, and ei is the evaluation of outcome i. Of course, individuals are not expected actually to perform the mental calculations described by this expectancy-value (EV) model. The model is taken not as an accurate description of the way in which decisions are made but rather as an ideal or normative model against which actual judgments and decisions can be compared. It is assumed that human decisions can be modeled as if a person were performing the stipulated calculations. Moreover, once an attitude has been formed, it is accessible in memory, and as indicated above, depending upon the behavior in question, it may or may not have a directive influence on that behavior.
Just as attitudes follow automatically from beliefs, so to do perceptions of social pressure and of control. That is, the more one believes that specific others are (or are not) performing the behavior and the more one believes that specific others think one should (or should not) perform the behavior in question, the more social pressure one will feel (or the stronger the perceived norm) with respect to performing (or not performing) the behavior. Similarly, the more one perceives that one can (i.e., has the necessary skills and abilities to) perform the behavior, even in the face of specific barriers or obstacles, the stronger will be one's perceived control or self-efficacy with respect to performing the behavior.
It is at the level of underlying beliefs that the substantive uniqueness of each behavior comes into play. For example, the barriers to using and/or the outcomes (or consequences) of using a condom for vaginal sex with one's spouse or main partner may be very different from those associated with using a condom for vaginal sex with a commercial sex worker or an occasional partner. Similarly, the beliefs about going to a women's clinic for a mammogram may be very different from beliefs about going to a university hospital or a private hospital, and the beliefs about taking an antidepressant may be very different from beliefs about taking a diuretic. Yet it is these specific beliefs that must be addressed in an intervention if one wishes to change intentions and behavior. And although an investigator can sit in her or his office and develop measures of attitudes, perceived norms, and self-efficacy, she or he cannot explain what a given population (or a given person) believes about performing a given behavior. Thus one must go to members of that population to identify salient outcome, normative, and control beliefs. To put this somewhat differently, one must understand the behavior from the perspective of the population one is considering.
Finally, Figure 1 also shows the role played by more traditional demographic, personality, attitudinal, and other individual difference variables (such as perceived risk, moods, and emotions). According to a reasoned action approach, these types of variables play primarily an indirect role in influencing behavior. For example, while men and women may hold different beliefs about performing some behaviors, they may hold very similar beliefs with respect to others. Similarly rich and poor, old and young, those from developing and developed countries, those who do and do not perceive they are at risk for a given illness, those with favorable and unfavorable attitudes toward family planning, and so forth may hold different attitudinal, normative, or control beliefs with respect to one behavior but may hold similar beliefs with respect to another. Similarly, exposure to an intervention or a media campaign may or may not produce changes in an individual's beliefs. Thus, there is no necessary relation between these “external” or “background” variables and any given behavior. Nevertheless, external variables such as cultural differences, moods, and emotions and differences in a wide range of values should be reflected in the underlying belief structure. For example, it is well known that, in comparison to being in a bad mood, when one is in a good mood, one is more likely to believe that a given course of action is more likely to succeed and that “good things” will happen. Similarly if one is mad or angry, one is less likely to believe that “good things” will happen, and in addition, one is likely to have less positive or more negative evaluations of possible outcomes than is someone who is happy or relaxed.
One advantage of a reasoned action approach is that it helps explain why different background factors are related (or are not related) to a given behavior. For example, if men are found to be more likely to get colonoscopies than women, a reasoned action approach should be able to explain why this is the case. That is, we should be able to identify the factors that are responsible for the different behaviors of men and women. For example, suppose both men and women had unfavorable attitudes toward getting a colonoscopy but felt considerable social pressure to do so. One possible explanation of the differential prevalence of this behavior in men and women could be that this behavior was driven primarily by normative considerations in men but by attitudinal consideration in women. On the other hand, suppose that we found that while this behavior was primarily driven by attitudinal considerations in both men and women, men had more favorable attitudes toward “getting a colonoscopy” than did women. This would suggest that men and women had different behavioral beliefs about getting a colonoscopy. Further examination might reveal that while men believed that getting a colonoscopy could actually prevent colon cancer, women did not hold this belief. This would suggest that an appropriate intervention for women would be to address this belief.
To illustrate how the theory can be used to design interventions, consider a study that was designed to examine the role of attitudes, social pressure, and perceived behavioral control as determinants of 6 different cancer-related behaviors.33 The items assessing IM constructs were embedded within a larger survey regarding seeking and scanning for cancer-related information. Each participant responded to 6 questions that measured IM components for each of the 6 behaviors of interest: getting a mammogram, colonoscopy, and prostate-specific antigen (PSA) test, exercising regularly, eating fruits and vegetables, and controlling one's diet to lose weight. Participants were 1753 individuals (874 male, 879 female) ranging in age from 40 to 70 years, with an average age of 52.77 (SD = 8.42) from a nationally representative US sample. With respect to race/ethnicity, 76.3% were white non-Hispanic, 11.1% were black non-Hispanic, 7.1% were Hispanic, 3.0% were identified as more than 2 races, and 2.6% indicated “other.” Participants responded to a questionnaire containing questions assessing intentions, attitudes, perceived normative pressure, and perceived behavioral control regarding cancer screening and healthy lifestyle behaviors. Specifically, all participants responded to questions regarding getting a colonoscopy in the next year (or when it is next recommended), eating 5 or more servings of fruits and vegetables most days in the next year, dieting to control weight, and exercising at least 3 times in most weeks over the next year. Male participants also responded to questions regarding getting a PSA test for prostate cancer in the next year (or when it is next recommended), and female participants responded to additional questions about getting a mammogram in the next year (or when it is next recommended). These items were embedded in a larger survey examining cancer-related information seeking and scanning34 that took place between October 2005 and June 2006.
Table 1 shows the variance accounted for and the standardized regression weights of attitudes, perceived control, and normative pressure as independent predictors of intentions to engage in each of the 6 behaviors.
Perhaps the first thing to notice is that the consideration of attitudes, normative pressure, and perceived control significantly predicted intentions to engage all 6 behaviors, accounting for between 44% to 54% of the variance. But perhaps more important, consistent with expectations, the relative importance of the 3 variables differed as a function of the behavior being considered. While all 3 variables contributed significantly to the prediction of most behaviors, normative pressure had very little influence on the intention to exercise. In marked contrast, normative pressure was by far the most important determinant of intentions to get a colonoscopy or to take a PSA test. What this suggests is that while an intervention designed to increase normative pressure to get a colonoscopy could be effective (e.g., if it actually did increase normative pressure), an intervention designed to increase normative pressure to exercise (even if it successfully did increase perceived pressure to exercise) is unlikely to influence exercise behaviors.
As another example, consider adolescents’ intentions to engage in vaginal intercourse in the next 12 months. These data come from the first year of a 3-year longitudinal study designed to investigate the impact of the media on adolescent sexual behavior. The sample is composed of 522 adolescents, 43% white and 41% black, 60% female, with equal numbers of 14, 15, and 16 year olds. As part of the survey, respondents were asked to indicate their behavioral, normative, and control beliefs about engaging in sexual intercourse in the next 12 months, as well as their intentions, attitudes, perceptions of normative pressure, and perceptions of perceived behavioral control with respect to this behavior. Consistent with the findings concerning cancer-related behaviors, attitude, norms, and perceived control explained 55% of the variance in intentions to have sex in the next 12 months. However, in contrast to the findings concerning colonoscopy, the intention to engage in vaginal sex is primarily determined by attitudinal considerations. More specifically, the standardized regression weights for attitudes, norms, and perceived control are .53, .22, and .07, respectively. This implies that the most effective intervention to reduce the likelihood that adolescents will engage in premarital sex in the next year would be one directed at decreasing the adolescents’ attitudes toward this behavior.
However, as indicated above, in order to do this, it will be necessary to change the adolescents’ beliefs about the consequences of engaging in this behavior. But which beliefs should be changed? As part of a pilot study, the adolescents’ salient beliefs about engaging in vaginal sex in the next 12 months were identified and were used to develop part of the closed questionnaire described above. Consistent with an EV formulation, the sum of the behavioral belief by outcome evaluation (b × e) products was correlated .71 with the direct measure of attitude. This provides strong support for the notion that we were able to identify the beliefs underlying the adolescent's attitudes toward engaging in sex. In order to develop an intervention, however, we need to know which of these beliefs distinguish between those who do and do not intend to engage in sex in the next 12 months. Table 2 shows the differences in behavioral beliefs between intenders and nonintenders as well as the correlation between each belief and the intention to have sex.
It can be seen that each of the 14 modal salient beliefs were significantly correlated with the intention to have sex, with intenders significantly more likely than nonintenders to believe that “good” outcomes would occur and that bad outcomes would not. Thus, if we want to reduce the adolescent's intentions to have vaginal sex in the next 12 months, we can either increase beliefs that engaging in sex will lead to negative outcomes or decrease beliefs that engaging in sex will lead to positive outcomes. Note, however, that this is not quite as simple as it sounds. If someone has had sex in the past, and believes that having sex will give them pleasure, please their partner, and increase their intimacy with their partner, it seems very unlikely that one will be able to develop an intervention to change these beliefs. Generally speaking, it will be difficult, if not impossible, to change beliefs that are based on direct experience. It may be possible however to craft an intervention that could successfully increase their beliefs that engaging in sex in the next year will lead to an increased risk of a sexually transmitted disease (STD) or pregnancy.
Generally speaking, interventions should address beliefs that are significantly related to the behavior in question. In addition, as Hornik and Woolf35 have argued, one also wants to address beliefs when there are enough people who do not hold the “appropriate” belief. That is, one wants to make sure that the intervention will change the beliefs of a large segment of the target audience. And finally, and in some ways most important, one wants to address beliefs that are “changeable.” As Hornik and Woolf35 have suggested, one should be able to craft a convincing message—one supported by reasonable arguments and, if possible, hard data.
What I have tried to show is that theories of behavioral prediction help us identify the critical behavioral, normative, or control beliefs that must be addressed if one wishes to reinforce or change any given behavior. But unfortunately, with the possible exception of Bandura's work on increasing self-efficacy,36 behavioral prediction and behavior change theories do not tell us how to reinforce or change those beliefs! Indeed, I think the biggest challenge we currently face is figuring out how to design communications or other types of interventions that will successfully change or reinforce these beliefs.
It is somewhat surprising that despite all the work that has been done on communication and persuasion, we still know very little about the factors that influence why someone will accept or reject a given argument or piece of information. One immediate implication of this is that it is critical that we very carefully test our interventions before we try to implement them in any population. If someone gave another person a chemistry set, that other person would not go down to his basement, mix a few chemicals together, and then go out and start vaccinating people. But I am willing to bet that many people have sat in their office or around a table with some colleagues, have put together what they thought was a brilliant intervention, and then went out and implemented it in an attempt to change some behavior in some population. Unfortunately, as we all know, many interventions are not only ineffective but often have deleterious effects. Just as one cannot “throw together” a vaccine, one cannot “throw together” an intervention. The implication is that one should never send a communication or intervene in some population without first carefully pre-testing the message or the intervention.
In conclusion, let me suggest that we do know what we have to do in order to change a behavior. That is, we can identify the beliefs that would have to be changed or strengthened in order to change or reinforce a given behavior. In that sense, we really do not need “new” behavioral theories. What we do need, however, is for people to better understand and to correctly use existing theory. Even more important, we need better theories of communication effects. In particular, we need to understand the factors influencing whether a given piece of information will be accepted or rejected. Whoever figures this out will make a real contribution to improving the public's health!
This publication was made possible by NCI Grant 5P50CA095856-04 and NICHD Grant 5R01HD044136-05. Its contents are solely the responsibility of the author and do not necessarily represent the official views of NCI or NICHD.
aNote that the phrase “one will or will not” is used because although these are logical complements of one another, they are not necessarily psychological complements; the reasons to perform an action are not necessarily the opposites of the reasons to not perform an action.
A reasoned action approach.
Standardized Regression Weights and Variance Accounted for in Each of 6 Cancer-Related Behaviors by Attitudes, Perceived Control, and Normative Pressure
| Behavior | Attitudes | Perceived Control | Normative Pressure | R2 |
|---|---|---|---|---|
| Mammography | .244 | .375 | .289 | .468 |
| Colonoscopy | .242 | .194 | .458 | .496 |
| PSA test | .240 | .224 | .422 | .496 |
| Exercise | .343 | .445 | .079 | .534 |
| Eating fruits and vegetables | .273 | .260 | .303 | .441 |
| Dieting | .338 | .342 | .245 | .537 |
Differences in Behavioral Beliefs between Intenders (n = 155) and Nonintenders (n = 371) about Having Sex
| Belief Held about Having Sex | Do Not Intend to Have Sex | Intend to Have Sex | Correlation with Intention |
|---|---|---|---|
| Give me pleasure | 0.36 | 2.30** | .482** |
| Improve relationship | −0.70 | 0.99** | .441** |
| Please partner | 1.05 | 2.17** | .335** |
| Increase intimacy with partner | 0.47 | 1.64** | .302** |
| Gain friends’ respect | −1.31 | −1.02 | .137* |
| Feel good about myself | −0.98 | 0.39** | .381** |
| Give me an STD | −0.79 | −2.00** | −.321** |
| Give me HIV | −0.98 | −2.20** | −.318** |
| Hurt relationship with partner | −0.81 | −1.98** | −.318** |
| Make parents mad | 1.55 | 0.59** | −.220** |
| Friends think badly | −1.11 | −2.25** | −.319** |
| Get pregnant | −0.92 | −1.58** | −.143** |
| Lose virginity | 1.80 | −0.55** | −.434** |
| Be taken advantage of | −1.00 | −2.49** | −.404** |
Gallery Theory Of Reasoned Action
 Theory Of Reasoned Action Theory Of Planned Behaviour By
Theory Of Reasoned Action Theory Of Planned Behaviour By
 The Theory Of Planned Behavior
The Theory Of Planned Behavior
 Let S Understand The Theory Of Reasoned Action Ajzen And
Let S Understand The Theory Of Reasoned Action Ajzen And
 Theory Of Reasoned Action Tra Technology Acceptance
Theory Of Reasoned Action Tra Technology Acceptance
 Pdf Intention To Experience Local Cuisine In A Travel
Pdf Intention To Experience Local Cuisine In A Travel
 Pdf Chapter 3 Theory Of Reasoned Action And Theory Of
Pdf Chapter 3 Theory Of Reasoned Action And Theory Of
 Videos Matching Theory Of Reasoned Action And Theory Of
Videos Matching Theory Of Reasoned Action And Theory Of
 Theory Of Reasoned Action Theory Of Planned Behavior Theory
Theory Of Reasoned Action Theory Of Planned Behavior Theory
 Theory Of Planned Behavior Wikipedia
Theory Of Planned Behavior Wikipedia
 Theory Of Reasoned Action 1health Behavior Chapter Ppt Download
Theory Of Reasoned Action 1health Behavior Chapter Ppt Download
 File Behavioral Process In Theory Of Reasoned Action Png
File Behavioral Process In Theory Of Reasoned Action Png
 Theory Of Reasoned Action Fishbein And Ajzen 1975
Theory Of Reasoned Action Fishbein And Ajzen 1975
Theory Of Reasoned Action Tra Theory Of
 Gale Academic Onefile Document The Theories Of Reasoned
Gale Academic Onefile Document The Theories Of Reasoned
 Theory Of Reasoned Action Tra Fishbein Ajzen 1975
Theory Of Reasoned Action Tra Fishbein Ajzen 1975
 Sage Reference The Theory Of Reasoned Action
Sage Reference The Theory Of Reasoned Action
 Sage Reference The Theory Of Reasoned Action
Sage Reference The Theory Of Reasoned Action
 Theory Of Planned Behavior Springerlink
Theory Of Planned Behavior Springerlink
 Predicting Substance Abuse Treatment Providers
Predicting Substance Abuse Treatment Providers
 Translating Theory Into Action A Focus On Smoking Cessation
Translating Theory Into Action A Focus On Smoking Cessation








0 Response to "Theory Of Reasoned Action"
Post a Comment